
Secondary Level of Use of Health Data in Europe

Adriatic team
The global pandemic of COVID-19 shook established social systems, but it was the use of data that played the leading role in coordinating cross-sectoral responses in the field of public health. However, we must not forget that even before the pandemic, optimization and modernisation of health systems were necessary. This is of particular relevance with regard to more efficient management of the limited resources required to cater for the needs of a growing and ageing population. Slovenia is among several European Union member states that are expected to face one of the largest increases in social expenditure relating to the ageing of the population, by 2060.
Where does Slovenia rank on the ODI (Open Data Institute) scale?
The Institute for Strategic Solutions, together with representatives from key organizations in the Slovenian healthcare system, validated a report on the secondary use of healthcare data in Slovenia; matrices were checked and updated based on the initial research into the Secondary use of Health Data in Europe and Slovenia’s ranking was estimated. We also exchanged views and opinions on the challenges and opportunities facing the stakeholders. Statistics is the language of science and our purpose was to translate the numerical results into words and to provide additional insight into the minds and attitudes of local medical experts.
The informative value of the report validation brings to the fore local insight into specific key areas, namely – infrastructure, capacity, innovation, justice, ethics and inclusion. All of which a modern and credible healthcare system in Slovenia is dependent on. The report is intended for key decision-makers in the field of healthcare, enabling them to discuss and implement new initiatives that will enhance the Slovenian healthcare system and make for a better future. The baseline survey was prepared by the Open Data Institute (ODI) and published in September 2021. Its main contributor was Mark Boyd. The ODI is an independent and not-for-profit consultancy founded in 2012 by Sir Tim Berners-Lee and Sir Nigel Shadbolt. The ODI offers training, research and strategic advice to organizations seeking to explore the applied value of data. It works from its headquarters in London, as well as through its global network of start-ups, members, and hubs. Its research report, The Secondary Use of Health Data in Europe, is based on the importance of the secondary use of health data in improving and enhancing the European health system of the future. The main theme of the research is based on the idea that transparent and trustworthy data systems relating to healthcare are the key to helping countries respond to the many challenges facing society and the economy. The vital question is, how well equipped are the individual countries of the European Union prepared for the transformation?
Secondary Level of Use of Health Data in Europe
The concept of the secondary use of data includes the utilisation and processing of data collected in medical records for efficient patient treatment – both for primary use at the doctor-patient level as well as using anonymized data to identify phenomena and trends. It can also play a key role in the development and planning of the health system through various analytical approaches and the grouping of data into meaningful data sets.
The authors of the initial research focused on several key areas, namely, infrastructure, capacity, innovation, equity, ethics and inclusion, all of which a modern and credible health system is based on. The research also identifies the main components and indicators of success that are necessary to optimize the health systems of individual EU countries from secondary level use of health data. In addition to the data that is created at the patient-doctor level i.e. the primary, secondary or tertiary level of health care, there is also the health data that individuals create for themselves, for example, daily activities, such as exercise and sleep levels. This is also very significant, however, even more important is the awareness that the aforementioned data can be anonymized and combined in a way that serves to identify phenomena and trends for more effective treatment leading to increased accessibility to good quality and safe health services. This all culminates in a more sustainable health system. The results of the baseline survey showed that European countries can be classified and organized into the four main groups shown below.
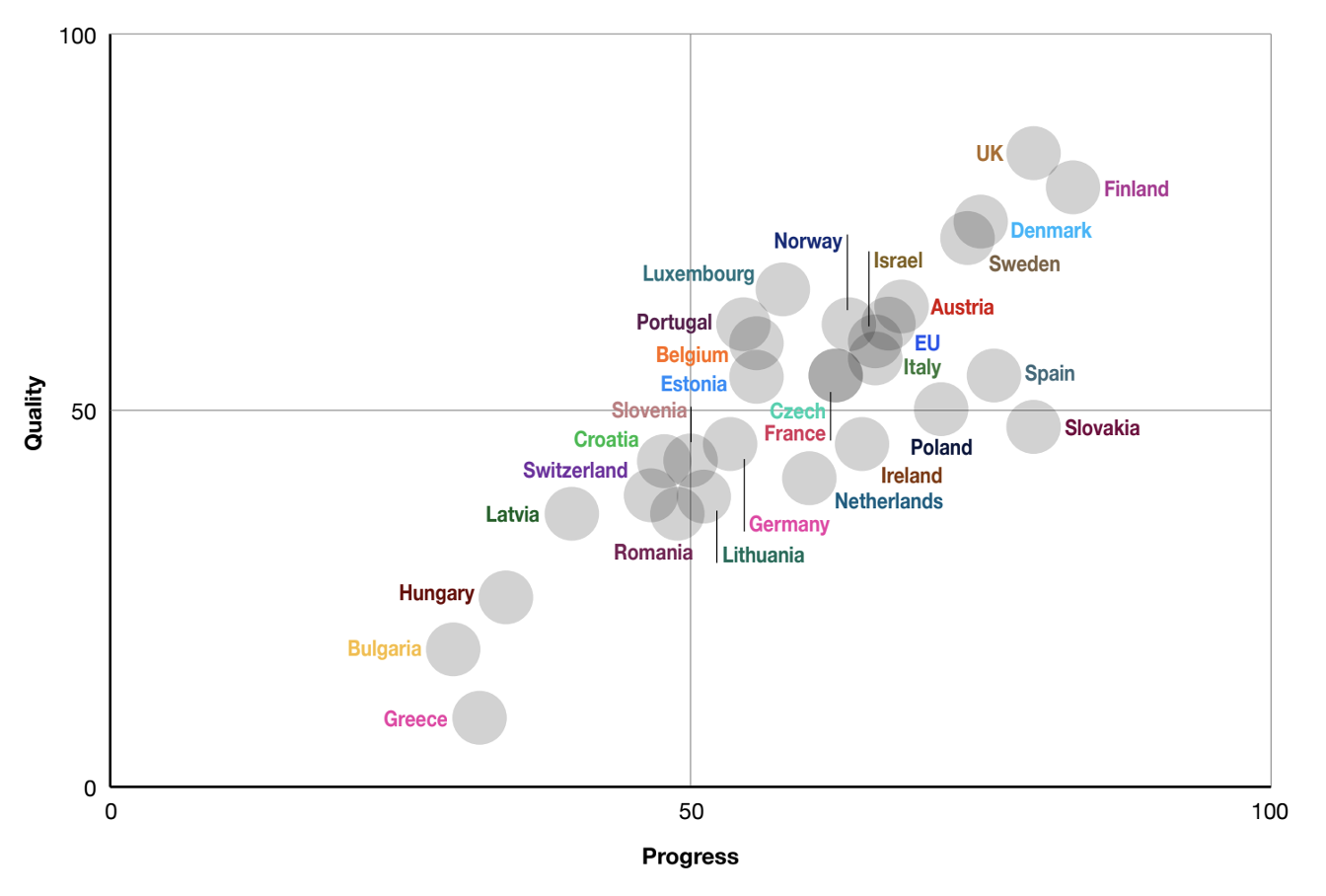
According to The Secondary Use of Health Data report, the ODI classified the countries into four groups, each group occupies a quadrant on the graph above:
Leading Countries: Policy quality is strong and the implementation level is advanced. This category includes Austria, Belgium, Czech Republic, Denmark, Estonia, European Commission, Finland, France, Israel, Italy, Luxembourg, Norway, Portugal, Spain, Sweden, and the United Kingdom.
Energy-constrained Countries: Policy quality is good, but the level of implementation is less advanced. None of the countries under consideration meet these criteria.
Countries with Limited Vision: The quality of policy is weak but the level of implementation is more advanced. This category includes Croatia, Ireland, Germany, Netherlands, Poland, and Slovakia.
Less Prepared Countries: The quality of policy is weak and the level of implementation is less advanced. This category includes Bulgaria, Greece, Hungary, Latvia, Romania, Slovenia and Switzerland.
Local Insights
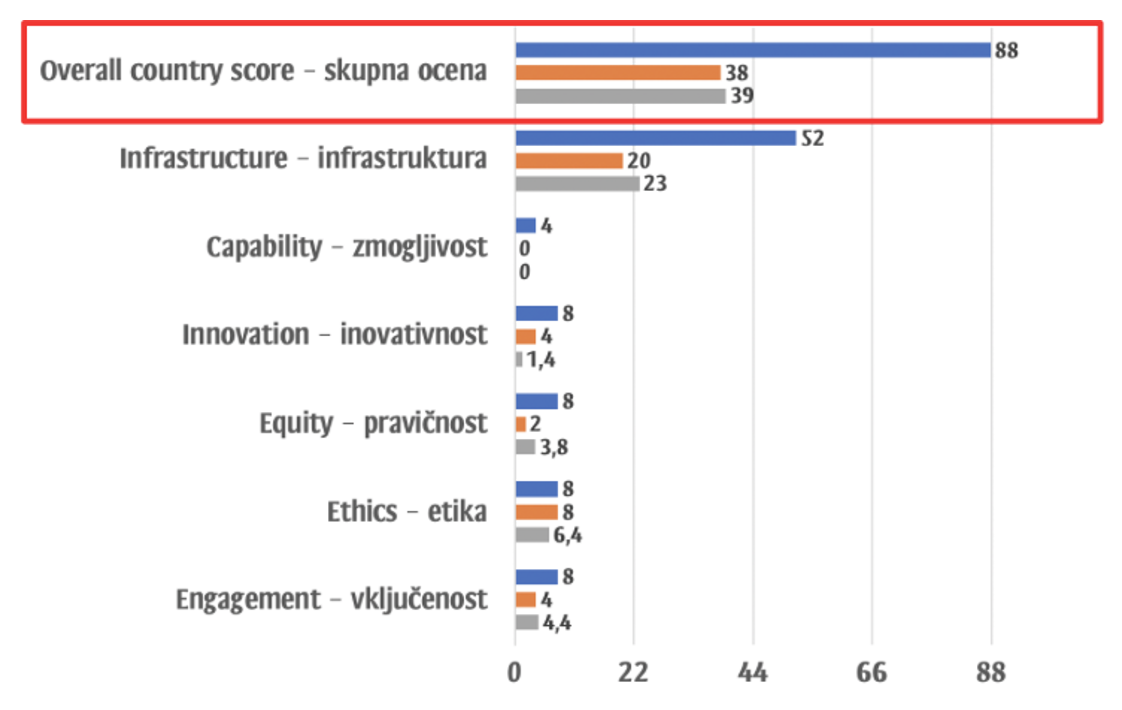
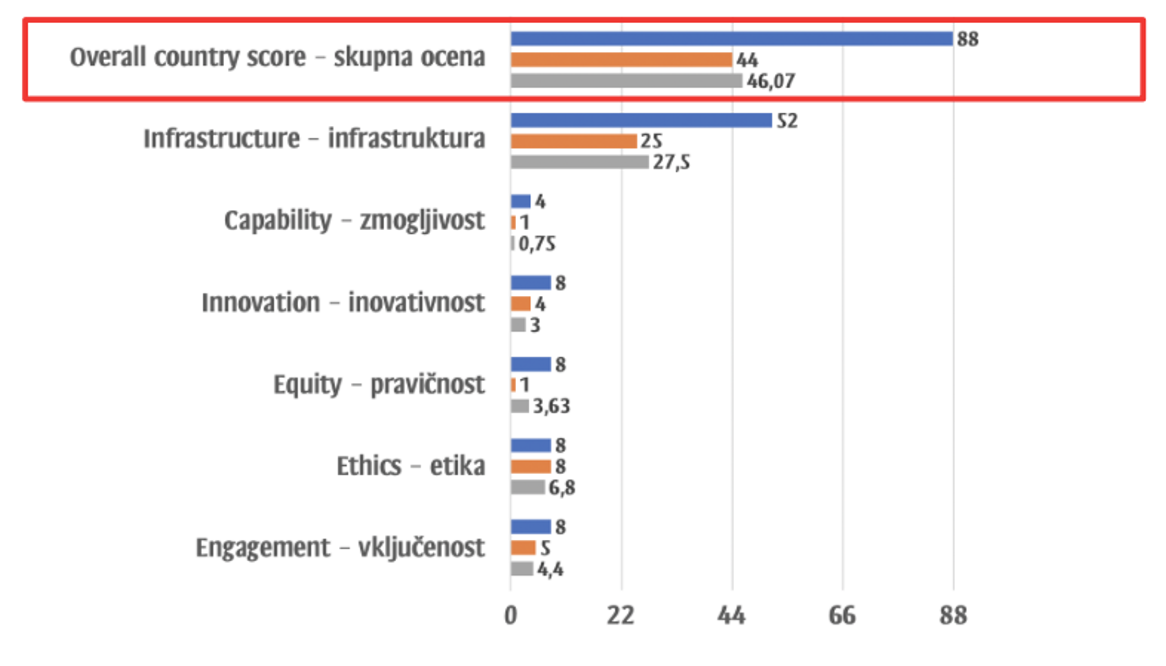
Individual interviews with key stakeholders who are part of the Slovenian healthcare system confirm the assessment attributed to Slovenia by the authors of the initial research into Secondary Use of Health Data in Europe. This is most noticeable in the absolute numbers we calculated as the statistical means of the ratings of the Slovenian experts interviewed. The overall assessment of the quality of Slovenian healthcare was 39 out of a possible 88, which is only slightly better than the ODI score, namely 38. Slovenian experts rated Slovenia better than the London researchers in the following categories – Infrastructure (23 versus 20 points out of a possible 52 points) and Justice (4 versus 2 points out of a possible 8 points). However, Slovenian experts rated Innovation worse than the London researchers (1 versus 4 points out of a possible 8 points). Slovenian experts also rated Ethics worse (6 points versus 8 points out of a possible 8 points), which is in line with international research in other areas. For example, in perceptions of corruption, domestic experts generally perceived more ethical slippages and violations than foreign observers. The Slovenian evaluators and evaluators from London gave the same ratings regarding the quality of Performance (both scored 0 out of a possible 4 points) and Inclusion (4 points out of a possible 8 points). As for the Implementation assessment, the overall assessment of Slovenian experts (46 points out of a possible 88 points) is only slightly better than the ODI assessment (44 points out of a possible 88 points). The average scores of Slovenian evaluators were better in the areas of Infrastructure (28 points versus 25 points out of a possible 52 points) and Justice (4 points versus 1 point out of a possible 8 points), but they were worse in terms of Innovation (3 points versus 4 points out of a possible 8 points), Ethics (7 points versus 8 points out of a possible 8 points) and Inclusion (4 points versus 5 points out of a possible 8 points). There were equal scores in the field of Capacity implementation (1 point out of a possible 4 points).
The openness to health data in Slovenia according to the ODI assessment compared to the average assessment of the Slovenian experts interviewed by the Institute for Strategic Solutions (ISR)
The state of implementation with regards to the openness of health data in Slovenia according to the ODI assessment compared to the average assessment of Slovenian experts
To summarise, there are encouraging signs that the Slovenian healthcare system is maturing in the context of effective use of the secondary level of data. However, the method in which the data is stored is still fragmented and a lot of work will be needed to get the secondary data infrastructure utilized to ensure an up-and-running strong and resilient healthcare infrastructure. Throughout the validation, Slovenian evaluators also expressed their own opinions regarding the international comparison, most specifically about which countries to look to in terms of good practice in the use of secondary data in healthcare, and identified Finland, Belgium, Sweden, Denmark, France and the Netherlands.







